Invasive BCIs as Treatment
Artificial Vision
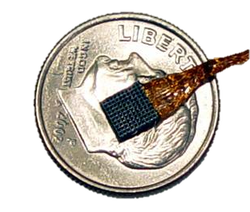 An array of 100 electrodes
An array of 100 electrodes
One of the earliest applications of invasive BCI technology was pioneered by private researcher William Dobelle. Dobelle devoted much of his life towards restoring sight for the blind through the development of an artificial vision system. His ultimate goal was to give blind patients “functional mobility” – the ability to perform everyday tasks and simple navigation unassisted. The first human trial occurred in 1978, when Dobelle implanted an array of 68 electrodes in the visual cortex of a blind man named Jerry. Dobelle was successfully able to transmit signals to these electrodes, stimulating the visual cortex and thereby producing the sensation of light in Jerry’s mind. In the context of artificial vision, sensations of light are simply referred to as phosphenes. The perception of phosphenes generated by the implanted electrodes provided Jerry with a rudimentary form of sight. In this first generation technology, phosphenes appeared in a limited field of vision and refreshed at a relatively low frame rate. It was far from restoring Jerry’s sight or providing him with functional mobility, but it was still a remarkable achievement
Shortly after Dobelle took these first steps, however, regulations caught up with him. In the infancy of invasive BCI, the Food and Drug Administration passed a series of amendments which ultimately prohibited the use of visual neuroprosthetics in humans. But the FDA wasn’t enough to stop Dobelle. He was able to bypass regulations by sending patients to Portugal for electrode implantation surgery. Dobelle continued refining his research for decades, until his death in 2004. By 2002, Dobelle’s artificial vision system had become far more portable than its first generation counterpart, which was constricted by the relatively primitive and bulky computers of the time. The later version consisted primarily of three parts: a camera attached to a pair of glasses, the brain implants themselves, and a signal processor attached to a belt. The signal processor, tuned specifically to the patient’s brain, was designed to translate images received from the camera into signals that the brain could readily interpret.
Shortly after Dobelle took these first steps, however, regulations caught up with him. In the infancy of invasive BCI, the Food and Drug Administration passed a series of amendments which ultimately prohibited the use of visual neuroprosthetics in humans. But the FDA wasn’t enough to stop Dobelle. He was able to bypass regulations by sending patients to Portugal for electrode implantation surgery. Dobelle continued refining his research for decades, until his death in 2004. By 2002, Dobelle’s artificial vision system had become far more portable than its first generation counterpart, which was constricted by the relatively primitive and bulky computers of the time. The later version consisted primarily of three parts: a camera attached to a pair of glasses, the brain implants themselves, and a signal processor attached to a belt. The signal processor, tuned specifically to the patient’s brain, was designed to translate images received from the camera into signals that the brain could readily interpret.
 Jens Naumann, using Dobelle's artifical vision system
Jens Naumann, using Dobelle's artifical vision system
Considering the remarkable complexity of the visual cortex, the electrical stimulation produced by implanted electrodes is comparatively crude. Nevertheless, the electrodes are indeed able to transmit useful and actionable information in the form of phosphenes. The phosphenes elicited by electrodes come in many forms, and by nature, they exist only in the mind of the beholder. They can appear as small points of light, or as squiggles, or as irregular blobs. In order to produce phosphenes that correspond to the physical world, it is important to map out the patient’s visual cortex, so that the different cortical regions can be appropriately stimulated. This is done by stimulating each of the BCI electrodes, one by one. Jens Naumann, a man blinded in each eye by two separate accidents, was the first to test drive Dobelle’s 2002 artificial vision system. Once the signal processor was successfully calibrated, Jens was able to discern basic shapes and to locate simple household items on a table. After gaining familiarity with his artificial vision, Jens was even able to drive a car at the annual American Society for Artificial Internal Organs conference.
As technology continues to advance, researchers hope to achieve even finer control over which neurons are stimulated, thereby leading to higher resolution phosphenes. Some experts believe that a 32 by 32 array of 1024 pixels would be sufficient to enable blind patients to perform most everyday tasks. Research is already underway to realize such devices, which contain an order of magnitude more electrodes than Dobelle’s latest design. This next generation technology hopes to bring patients like Jens even closer to complete functional mobility.
As technology continues to advance, researchers hope to achieve even finer control over which neurons are stimulated, thereby leading to higher resolution phosphenes. Some experts believe that a 32 by 32 array of 1024 pixels would be sufficient to enable blind patients to perform most everyday tasks. Research is already underway to realize such devices, which contain an order of magnitude more electrodes than Dobelle’s latest design. This next generation technology hopes to bring patients like Jens even closer to complete functional mobility.
Motor Neuroprosthetics

Motor neuroprosthetics are another promising application of invasive BCIs. These are systems which enable patients to control a robotic arm, or other external device, with their thoughts. This technology is largely aimed at patients with tetraplegia, who suffer from partial or complete paralysis. To accurately control a robotic limb requires the transmission of high quality signals from the brain, making invasive BCIs more suitable than non-invasive BCIs for this task. BrainGate, a motor neuroprosthetic developed by Cyberkinetics, is a leading product in this field. Like Dobelle’s artificial vision system, BrainGate consists of three fundamental components: an implant with electrodes, a decoder for interpreting the signals from the implant, and an external device with which to interface. The external device could be anything from a robotic limb, to a motorized wheelchair. In many ways, the underlying technology between Dobelle’s artificial vision system and Brain is similar. Perhaps one of the most significant differences is that the artificial vision system was designed to transmit information to the brain, from the external world, while BrainGate aims to transmit information from the brain, for the purpose of operating external equipment. A remarkable demonstration of BrainGate’s results can be seen in the video below.
Ethics of Invasive BCI
In examining the ethics of invasive BCI, safety is of paramount importance. In the early days, Dobelle’s main concern was that the BCI would easily become infected or would otherwise be rejected by the body. Fortunately, these risks proved to be low. For either an artificial vision system or a motor neuroprosthetic, electrodes can be reliably implanted in the brain without substantial risk of rejection. Of course, the surgery itself is an undeniably risky procedure, since the electrodes must be directly implanted onto the cortex. These risks are unavoidable with current technology, and so they simply must be accepted by any patients considering this radical treatment. For this reason, only patients suffering from a significantly incapacitating illness are currently considered for invasive BCI treatment. In the case of blindness and tetraplegia, the promising benefits of invasive BCI technology can offset these inherent risks posed by treatment.
For patients suffering less debilitating conditions, the ethical considerations are not so clear. At what point do the rewards justify the risks? As challenging as this question can be, it is certainly not unfamiliar territory for the medical industry. However, what distinguishes invasive BCIs, from an ethical perspective, is that treatment can become blurred with enhancement. Invasive BCIs could allow disabled individuals to surpass normal abilities, at least in certain respects. Conventional medical treatment attempts to restore a patient to a near-median level of health. Invasive BCIs, on the other hand, could skyrocket a patient well past the median. An amputee with a bionic arm would have distinct advantages over his fully biologically counterparts. Although a bionic arm might not exhibit the same fluidity of motion as a human arm, it could excel in strength and durability. These benefits may not be important for an average person, but they could be highly desirable for a construction worker.
The artificial vision system could exhibit similarly interesting tradeoffs as well, as the technology continues to develop. An artificial vision system might have inferior resolution to a human eye, while still exhibiting certain advantages. For instance, even with current technology, the artificial vision system could be modified to include cameras capable of detecting x-rays, or capable of zooming into objects far away. Though such use cases would be unusual, this modified system would give the patient a uniquely augmented sense of sight. Moreover, the artificial vision input needn’t originate in the physical world; the BCI could instead be used to project web pages and other virtual information. The resolution isn’t yet sufficient to support reading fine print, but that could change as the field of artificial vision continues to advance. In this way, artificial vision could promote an entirely novel form of digital consumption.
For patients suffering less debilitating conditions, the ethical considerations are not so clear. At what point do the rewards justify the risks? As challenging as this question can be, it is certainly not unfamiliar territory for the medical industry. However, what distinguishes invasive BCIs, from an ethical perspective, is that treatment can become blurred with enhancement. Invasive BCIs could allow disabled individuals to surpass normal abilities, at least in certain respects. Conventional medical treatment attempts to restore a patient to a near-median level of health. Invasive BCIs, on the other hand, could skyrocket a patient well past the median. An amputee with a bionic arm would have distinct advantages over his fully biologically counterparts. Although a bionic arm might not exhibit the same fluidity of motion as a human arm, it could excel in strength and durability. These benefits may not be important for an average person, but they could be highly desirable for a construction worker.
The artificial vision system could exhibit similarly interesting tradeoffs as well, as the technology continues to develop. An artificial vision system might have inferior resolution to a human eye, while still exhibiting certain advantages. For instance, even with current technology, the artificial vision system could be modified to include cameras capable of detecting x-rays, or capable of zooming into objects far away. Though such use cases would be unusual, this modified system would give the patient a uniquely augmented sense of sight. Moreover, the artificial vision input needn’t originate in the physical world; the BCI could instead be used to project web pages and other virtual information. The resolution isn’t yet sufficient to support reading fine print, but that could change as the field of artificial vision continues to advance. In this way, artificial vision could promote an entirely novel form of digital consumption.
